Guidance note on Female Genital Mutilation cases
This guidance note provides an overview of working within the Code of Practice when faced with complex and sensitive issues involving Female Genital Mutilation (FGM).
This guidance was reviewed in July 2024.[1] The law or procedure may have changed since that time and members should check the up-to-date position.
It is important to recognise that the Resolution Code of Practice must be read in conjunction with the professional duties imposed by regulators to act in the best interests of clients and to follow the Family Law Protocol when dealing with such cases.
Training and experience
If FGM becomes apparent as an issue within a case, we recommend that you consider whether you have sufficient experience for such cases. You should not undertake FGM work without the relevant training.
Resolution’s Specialist Accreditation scheme includes the opportunity for lawyer members to achieve specialist accreditation in this specialist area of practice.
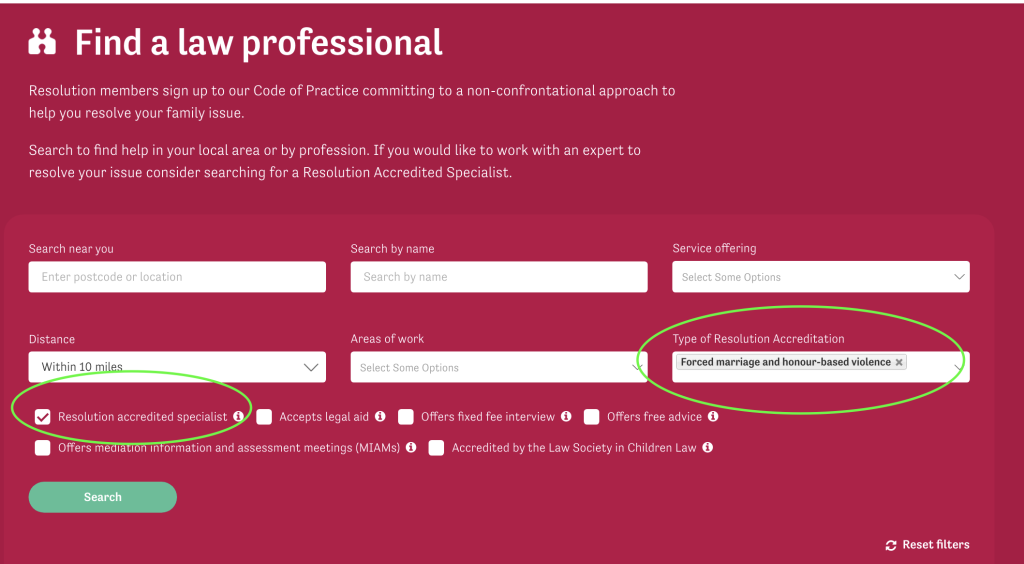
Members holding Specialist Accreditation in FGM can be found on the Resolution website, click on Find a law professional, then click on “Advanced Search”, then choose “Forced marriage and Honour-based violence” from the “Service offering” drop down box and tick the “Resolution Accredited Specialist” box
If you are unable to contact a specialist immediately, then it is vital that you contact the specialist FGM officer working within the Forced Marriage Unit (FMU) of the Home Office/Foreign and Commonwealth Office and be guided by them:
- telephone: 020 7008 0151
- email, including for outreach work: [email protected]
and/or one of the listed in the resources section below in order to ensure a that any individual has an immediate supporting link.
What is Female Genital Mutilation
Female genital mutilation (FGM) comprises all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons.
The World Health Organisation (WHO) has categorised FGM in to four major types:
“Type 1: This is the partial or total removal of the clitoral glans (the external and visible part of the clitoris, which is a sensitive part of the female genitals), and/or the prepuce/clitoral hood (the fold of skin surrounding the clitoral glans).
Type 2: This is the partial or total removal of the clitoral glans and the labia minora (the inner folds of the vulva), with or without removal of the labia majora (the outer folds of skin of the vulva).
Type 3: Also known as infibulation, this is the narrowing of the vaginal opening through the creation of a covering seal. The seal is formed by cutting and repositioning the labia minora, or labia majora, sometimes through stitching, with or without removal of the clitoral prepuce/clitoral hood and glans.
Type 4: This includes all other harmful procedures to the female genitalia for non-medical purposes, eg pricking, piercing, incising, scraping and cauterizing the genital area.”
The age at which a potential victim is vulnerable to FGM can vary widely from birth to adult life. It can occur during the postnatal period of pregnancy.
It used to be believed that FGM was a “one-off” procedure, but recent case history suggests this is not necessarily the case. The procedure may be repeated, often resulting in a different WHO category.
The law
While the WHO definition was not formally incorporated into the definition of FGM within Female Genital Mutilation Act (FGMA) 2003 s1(1), it was adopted by Sir James Munby, in the matter of Re B and G (Children) (No 2) [2015] EWFC 3.
Sir James Munby observed that knowledge and understanding of the classification and categorisation of the various types of FGM is vital and that the WHO classification is the one widely used for forensic purposes.
The majority of FGM cases will fall within either the public children’s law or the private children’s law jurisdiction, but it is important to note that FGM is also a criminal offence and has been since the Prohibition of Female Circumcision Act 1985 (now replaced by the Female Genital Mutilation Act 2003).
As with forced marriage, the availability of civil remedies is essential to victims/potential victims who do not wish to criminalise their family members, but do not wish to be abused in this way.
Safeguarding
The government has published multi-agency statutory guidance on female genital mutilation with guidelines for those with statutory duties to safeguard children and vulnerable adults. All members are advised to make themselves familiar with this document. (Published in 2016 and last updated in July 2020).
There is a FGM mandatory reporting duty of regulated health and social care professionals and teachers in England and Wales to the police and/or children’s services with disciplinary consequences if disclosure of “known” cases in under 18s if not made within one month of the professional becoming aware.
In addition, some professionals can be guilty of criminal offences if they are closely involved with children and ought to have known that they were at risk of FGM. This applies more to Cafcass, education and health practitioners and Children’s Services.
By the very nature of the issue, FGM happens in private, within families and is often hidden. It occurs in the United Kingdom as well as other parts of the world.
Cultural sensitivity
Cultural sensitivity on the part of the lawyer is absolutely essential. Although regarded as a form of child abuse, FGM is consistently regarded by those who practise it as an essential cultural/traditional/religious/necessity. It is not practised by parents who want to hurt their children, but by parents who genuinely believe that this is the right and only action to take for the benefit of their children and their future lives. Parents may often be under significant pressure within their own family or wider community to comply with what is regarded as a required to remain members of their family and/or local community.
You should therefore be very aware that when upholding issues of child and adult protection and safeguarding human rights, that you do so in a way that is sensitive and respectful to the culture of others.
Correspondence should be drafted in accordance with Resolution’s Good Practice Guide to Correspondence and should adhere to all standards of cultural sensitivity.
Talking to the client: cultural considerations
Whether the client is a potential respondent to a case or applicant or a protective party, you should bear in mind that in different countries and, indeed, different continents, the words “female genital mutilation” are rarely used.
Each country will have its own practice and within each country each tribe or ethnic group will have their own words. FGM is frequently used as a collective term for a range of procedures that involve partial or total removal of the external female genitalia for non-medical reasons. It is sometimes referred to as female circumcision, or female genital cutting.
Certain ethnic groups in Asian countries practice FGM, including in communities in India, Indonesia, Malaysia, the Maldives, Pakistan and Sri Lanka. In the Middle East, the practice occurs in Oman, the United Arab Emirates and Yemen, as well as in Iraq, Iran, Jordan, Somalia, Sudan, Algeria, Morocco and the State of Palestine. Forward UK have produced a map of the prevalence of FGM (of certain types) in the world.
Given the wide variety of words used by the different communities, you cannot be expected to know them all.
Annex G of the Government’s Multi Agency Guidance sets out a very useful list of terms used for FGM in other languages and The National FGM Centre also has a useful list of the common country/language-specific terms. However, it may not be comprehensive so you should ask the individual what word they use. In practice, most will understand the verb “to cut” and the practice promoted by “the cutter”.
See the Resolution FGM Screening and Awareness Information for more information.
Note on Islamic position on FGM
There is a misconception that FGM is part of Islam but FGM is not an Islamic obligation and the majority of Muslim scholars condemn it. In some communities, the term used for FGM is ‘Sunna’ (or recommended), which is a word referring to a practice following the traditions of Prophet Mohammed. However, the hadiths (narrations of Prophet Muhammad’s sayings) this has been based on have been shown to be inauthentic in fact this stance contradicts strong principles in Islam that forbids mutilating the body. FGM is a practice which predates Islam and is practiced by communities of various faiths and no faith. However, Muslims who practice FGM try and wrongly rationalise it as an Islamic religious practice even though it predates Islam and is not practiced by the majority of Muslims globally.
International elements to FGM cases
It is essential to be aware that parents may attempt to remove or abduct their child from jurisdiction so that FGM can be performed in another part of the world where this procedure is more readily available and is not criminalised.
It is recommended again that if you do not have the necessary experience of international family law cases or of child abduction matters that you should seek urgent professional assistance.
In Fornah v Secretary of State for the Home [2005] EWCA Civ 680 Auld LJ described FGM as a practice that is “internationally condemned and in clear violation of Article 3 of the European Convention for the Protection of Human Rights”. The judgment was in respect of an appeal against the Secretary of State’s refusal to grant asylum to a then 15-year-old girl.
Lord Justice Auld went on to observe that FGM is not peculiar to Sierra Leone but is so “widespread there and so bound up in the culture and traditions of that country at all levels that it causes difficulties in claims for asylum by young Sierra Leonean girls who fear it”
Section 70 of the Serious Crime 2015 Act amends FGMA 2003 s4 and makes provision for extending the prohibition on FGM to acts done outside the jurisdiction. The legislation therefore captures offences of FGM committed outside of the jurisdiction by or against those who are at the time habitually resident in the United Kingdom irrespective of whether they are subject to immigration restrictions.
Confidentiality
Lawyers have a duty to other organisations and there are occasions when their duty of confidentiality to a client can be overridden. The lawyer is an officer of the court and a gatekeeper of public funding and must be alert to incidents of criminal activity, which may mean that they are faced with the difficult decision about breaking their confidentiality to their own client. This is particularly true in cases of FGM.
Ensure that you inform your clients at an early stage that there may be incidents when confidentiality has to be overridden. This includes reminding clients of your duty to the court, the Legal Aid Agency and potential duty to the police and social services of criminal activity, especially if a threat to a child or children is discovered. Please think carefully about how you will explain these duties in a way that doesn’t overwhelm any client, prevent them from feeling able to disclose, is understandable to them and is reassuring rather than threatening. It should be explained in a way that is clear and sets out your aim (and your duties) to do what you can and must to protect them and/or their child/ren.
The SRA ethics helpline can assist in this area. Call them on 0370 606 2577 or email them at [email protected]
In addition, under the terms of the Serious Crime Act 2015, which introduces amendments to the FGMA 2003, confidentiality to victims and potential victims is guaranteed by law save for in very exceptional circumstances. Refer to this legislation if you are in any doubt.
Expert witnesses
At the present time there is no definition of an expert witness in relation to FGM and witnesses are being identified on a case-by-case basis. The Family Justice Board is, however, attempting to identify and provide criteria, in order to create a list of expert witnesses.
In the family courts anthropologists, sociologists as medical experts such as paediatricians (with particular expertise on FGM) have previously been instructed.
The Ministry of Justice is aware that people who would have the necessary cultural or medical knowledge may not be prepared to advise or report at legal aid rates. You should look to a prior authority if rates are to be exceeded in each case.
Litigants in person
Please read the Good Practice Guide to Working with Litigants in Person.
Specific issues relating to legal aid
You should keep up to date with legal aid policy and provide information to your clients about its availability in these types of matters, even where your firm is unable to provide legal aid assistance.
Female Genital Mutilation (FGM) cases in private law do not fall within the Family Advocacy Scheme (FAS) but are treated in the same way as forced marriage protection cases. The costs are recorded on an hourly rate rather than a fixed fee.
Legal aid is available when represented in a FGM Protection Order matter and there are no court fees in applying for an FGMPO. For more information see Gov.uk here.
Child abduction
Your client may be able to get legal aid if your child has been unlawfully removed within the UK or from the UK (or there is a risk of that): https://check-your-client-qualifies-for-legal-aid.service.gov.uk/. The legal aid checker for the public is here.
For more assistance you can contact a Resolution specialist accredited child abduction lawyer, or contact the International Child Abduction Contact Unit (ICACU) and Reunite international who support both abducting and left behind parents.
Summary
FGM is an area of intense cultural and personal sensitivity and often legal complexity. It is essential that members abide by the Code of Practice and the Good Practice Guides at all times.
You should:
- Act professionally at all times. Matters of this kind should also be handled sensitively whilst retaining a level of objectivity.
- Be aware and/or careful that any action/s you are considering or take do not result in effectively colluding in any way with a client. Your aim must be to afford appropriate protection, advice and support, including that individuals have an appropriate ‘next step’ in terms of continuing support (see resources listed below).
- Draft Resolution-compliant letters and documents.
- Act promptly when faced with the threat or reality of FGM and consider if there are immediate safeguarding issues which need to be put in place concerning immediate danger to health and bodily integrity and/or removal from the jurisdiction, which is also a child protection matter (please refer to Resolution’s Good Practice Guide to Safeguarding Children and Young People).
If in any doubt, seek expert help and advice reflecting this very complex and sensitive area of law.
Resources
Guidance
- Gov.uk Multi-agency statutory guidance on female genital mutilation
- Gov.uk Female Genital Mutilation Resource Pack
- The Law Society, The Family Law Protocol
- Resolution FGM Screening and Awareness Information
- Resolution Guidance Note on Instructing experts in proceedings involving children
- Resolution Good Practice Guide to Safeguarding Children and Young People
- FGM Guidance for Schools National FGM Centre (2019)
Publications
- Tackling female genital mutilation in the UK Current response is disproportionate and should be reconsidered, Sarah M Creighton, Zimran Samuel, Naana Otoo-Oyortey and Deborah Hodes [BMJ 2019;364:l15 doi: 10.1136/bmj.l15 (Published 7 January 2019).
- Cut: One Woman’s Fight Against FGM in Britain Today, Hibo Wardere, Simon & Schuster Ltd (2016)
- A Barrister’s Perspective on the Challenges of Applying for FGM Protection Orders, Dr Charlotte Proudman, National FGM Centre
Organisations
Africans Unite against Child Abuse (AFRUCA)
Promotes the rights and welfare of African children with the belief that culture and religion should never be a reason to abuse children.
Tel (London): 0207 704 2261
Tel (Manchester): 0161 205 9274
Email: [email protected]
FGM Clinic at University College London Hospital
The Forced Marriage Unit
The Forced Marriage Unit (FMU) is a joint Foreign and Commonwealth Office and Home Office unit that leads on the government’s forced marriage policy, outreach and casework.
Tel: 0207 008 0151
Email: [email protected]
Foundation for Women’s Health Research and Development (FORWARD)
An organisation that promotes gender equality and safeguarding the rights of African girls and women, specifically in FGM, Child Marriage and Obstetric Fistula practice.
Tel: 0208 960 4000
Email :[email protected]
Health and Social Care Information Centre Female Genital Mutilation Datasets
Imkaan
Imkaan is a UK-based, black feminist organisation dedicated to addressing violence against women and girls.
Tel: 0207 842 8525
Email: [email protected]
Iranian and Kurdish Women’s Rights Organisation (IKWRO)
An organisation that aims to protect Middle Eastern and Afghan women and girls who are at risk of ‘honour’ based violence, forced marriage, child marriage, female genital mutilation and domestic violence and to promote their rights.
Tel: 0207 920 6460
Local safeguarding children’s boards
Many local authorities have resources and procedures for professionals dealing with FGM
National FGM Centre
Funded by the Department for Education, the National FGM Centre provides specialist social care provision on FGM, alongside a knowledge hub with quality-approved resources for frontline professionals and a community-based prevention programme.
Tel: 208 498 7137
NSPCC guidance on FGM
Including dedicated FGM helpline by email [email protected] and telephone 0800 028 3550
[1] Resolution would like to thank Professor Zimran Samuel of Doughty Street Chambers and LSE for his assistance in reviewing and updating this guidance note. We also note the input and work of Cris McCurley and Angela Lake-Carroll in the initial drafting of this guidance and to Dr Naheed Ghauri for additional comments.